Certainty
in real-time
Professor Dr. Gian Franco Veraldi is developing a future-oriented minimally invasive treatment for cardiovascular diseases at the University Hospital of Verona. With the help of a 3D C‑arm from Ziehm Imaging, he can obtain certainty during surgical interventions, thus avoiding revisions and shortening hospital stays for patients.
Between the first surgical repair of an abdominal aortic aneurysm (AAA) and today lie almost 70 years. For a long time, the only solution for the often-life-threatening malformations of the aorta was a complicated open surgical procedure. Currently, more and more doctors are advocating minimally invasive treatment of aortic aneurysms. For patients, the new method is much gentler: less blood loss, improved wound healing, and reduced cardiovascular insufficiencies shorten hospital stays in most cases.
Reliable. Fast. Gentle.
Minimally-invasive vascular surgery
Professor Dr. Gian Franco Veraldi is an expert in this modern method of vascular surgery. With more than 8,000 surgical procedures and a professorship for vascular and cardiac surgery at the University of Verona, he is in high demand, and he radiates professionalism in his daily work: relaxed but concentrated. Today, together with his assistant Dr. Marco Macrì, he is preparing for a minimally invasive treatment of AAA. The patient is in his late 60s and is a high-risk patient. He had a stent implanted several years ago that now has to be extended with a stent connection to treat another aneurysm. For Prof. Dr. Veraldi, the minimally invasive procedure is a sound and important alternative to an open operation. “More than 60 percent of our operations are minimally invasive, i.e., endovascular aortic repair (EVAR). This is the more reliable alternative for us, especially for older patients, as it is gentler and, more importantly, faster than open surgery,” says Prof. Dr. Veraldi.
Continuous real-time monitoring
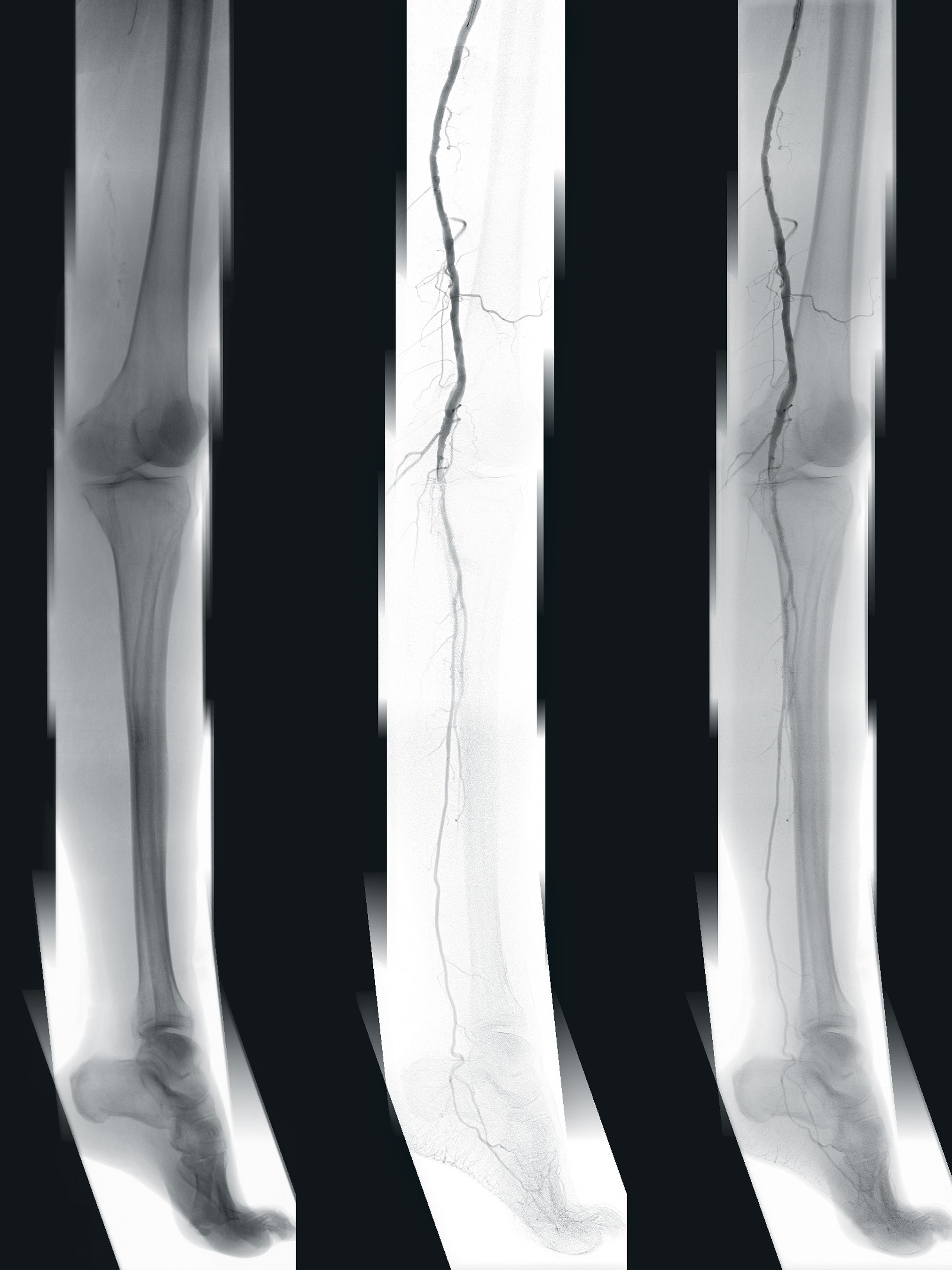
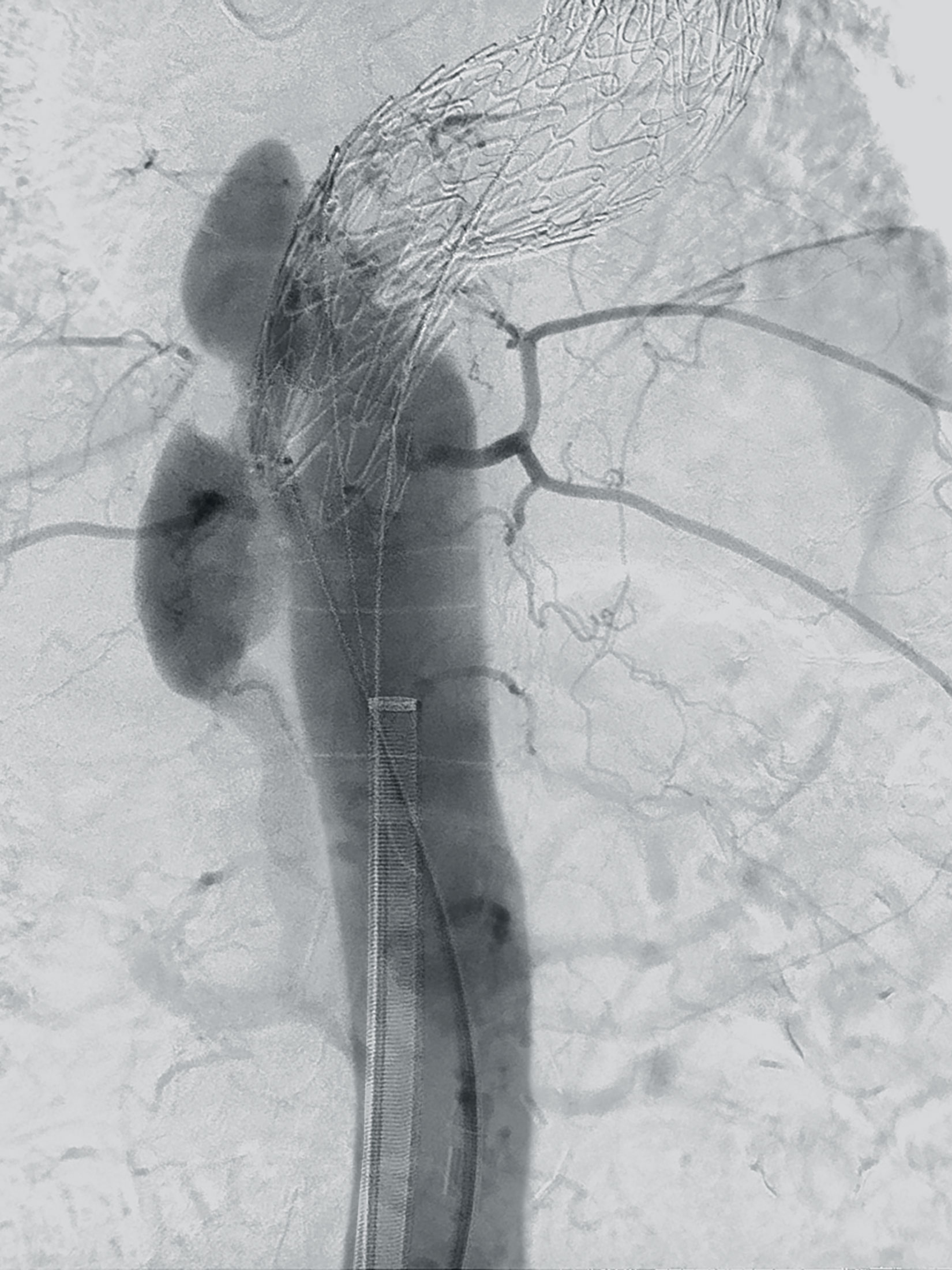
He and his team have been using the Ziehm Vision RFD 3D CMOSline1 since early 2019. Although the 3D C‑arm was originally designed for complicated procedures in orthopedics, traumatology, and spinal surgery, with its high-resolution 2D imaging capabilities it is equally suitable for multidisciplinary use in vascular surgery and angiography. Prof. Dr. Veraldi therefore operates on the aneurysm with the new C‑arm in the usual way for the time being; he does not have to change his routine procedure. The stent graft is introduced via the pelvic arteries into the aorta using a catheter system while under constant 2D X‑ray control. Prof. Dr. Veraldi places the stent in the affected vascular section – precise to the millimeter. For optimum adaptation and sealing of the prosthesis in the vessel, the stent is pressed against the aortic wall using a dilatable balloon. It is particularly important that the renal arteries are not covered by the stent in order to maintain supply to the organ, and that a piece of the new implant overlaps the existing stent.
“The combination of high-end 2D imaging and innovative intraoperative 3D stent control in one system allows us to optimize proven surgical techniques in the field of vascular surgery.”
In the past, the usual method of intraoperative control angiography often did not give Prof. Dr. Veraldi the assurance he needed, and he had to rely on his experience. Normally, he would have been able to close the patient following a final contrast agent angiogram. After a few days a postoperative CT would have been performed to check the location, the correct opening of the stent, and whether there was sufficient blood supply to the aorta and adjacent vessels. If the postoperative exam had shown that something was not 100 percent correct, the patient would have had to undergo a corrective intervention. “This was always unsatisfactory for me,” says Professor Dr. Veraldi. “The postoperative CT scan to verify the result of the operation is still considered the gold standard today. However, it does not give us any certainty during the procedure that our work has been successful.”
“In the past, after stent placement and the final contrast angiogram, we had to wait days for the postoperative CT. This was always unsatisfactory for me. Today we proceed differently. After the placement of the stent, we perform an intraoperative 3D scan, which gives us the opportunity to check. If necessary we can immediately make improvements.”
“Today, in three out of four cases, thanks to intraoperative 3D monitoring, we adjust our treatment strategy during the operation. This will reduce the number of revision operations and shorten hospital stays.”
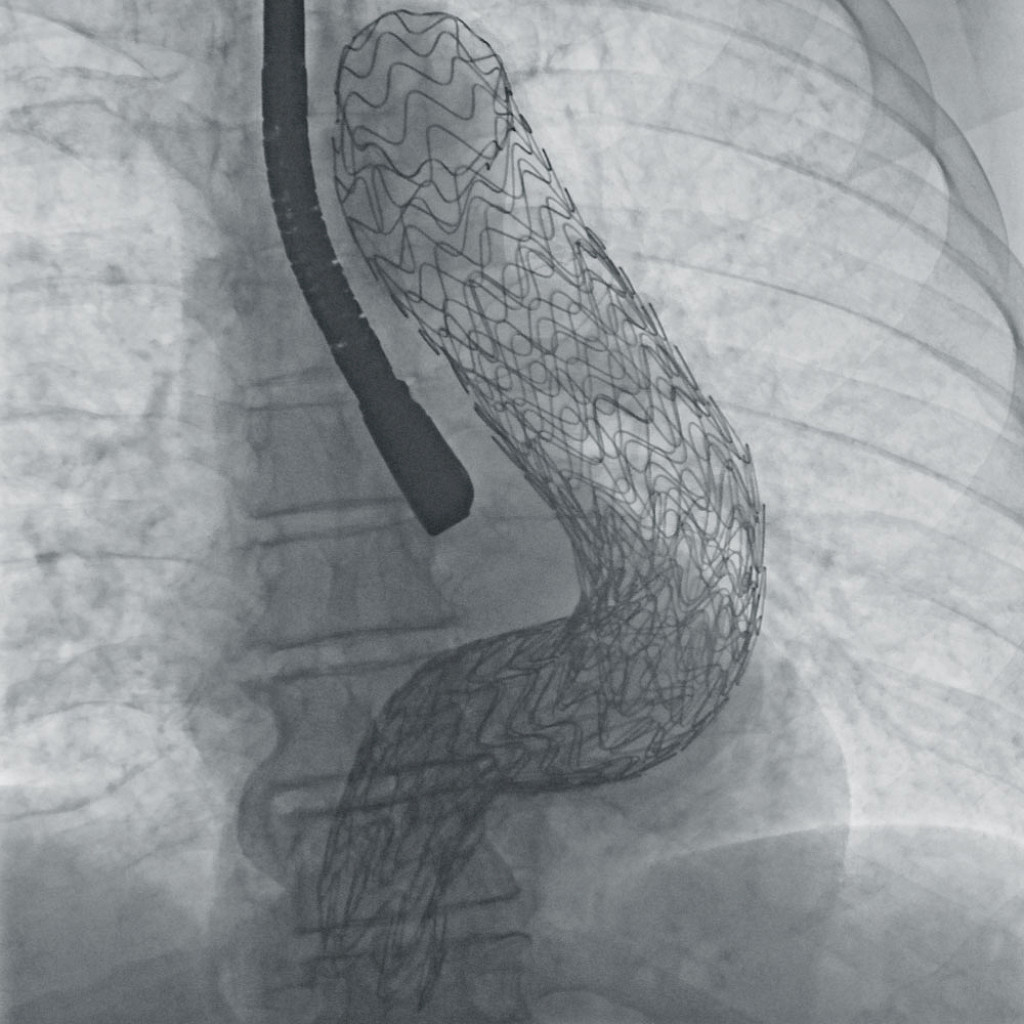
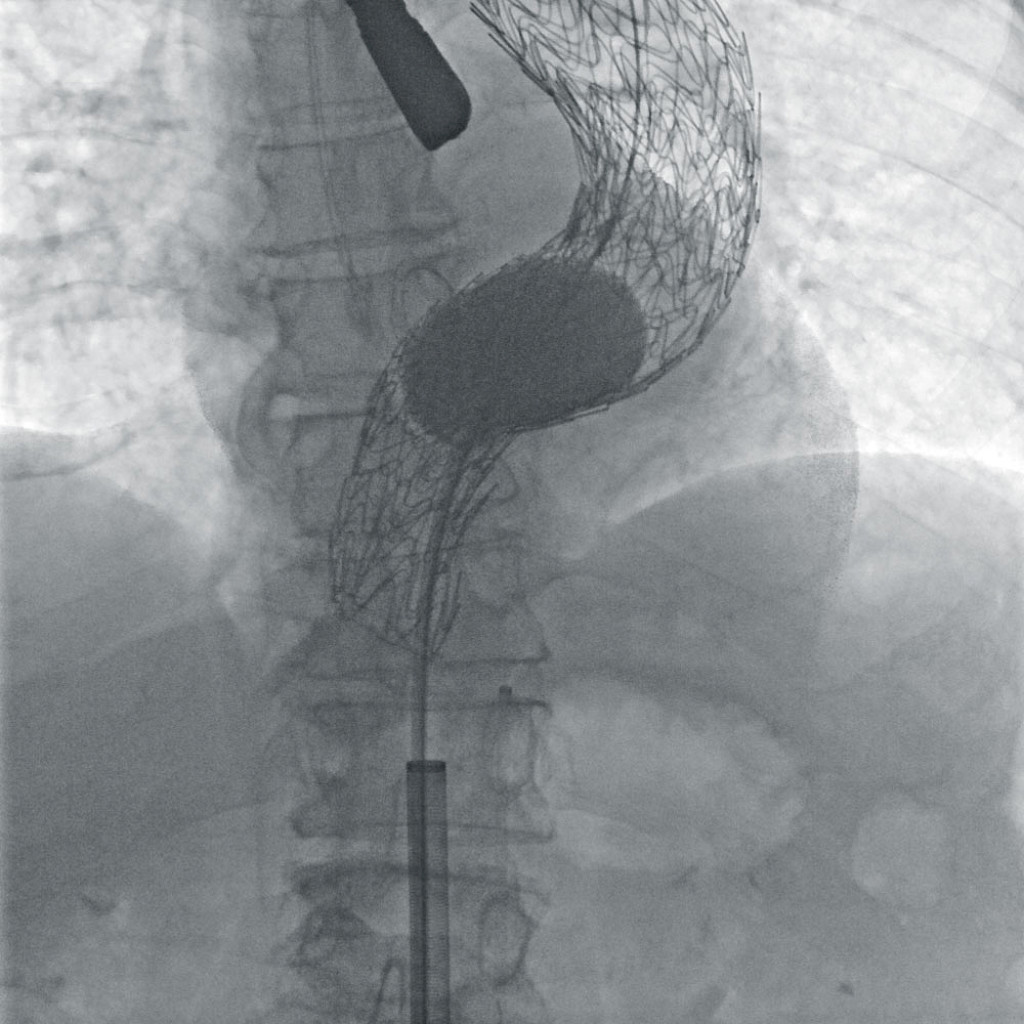
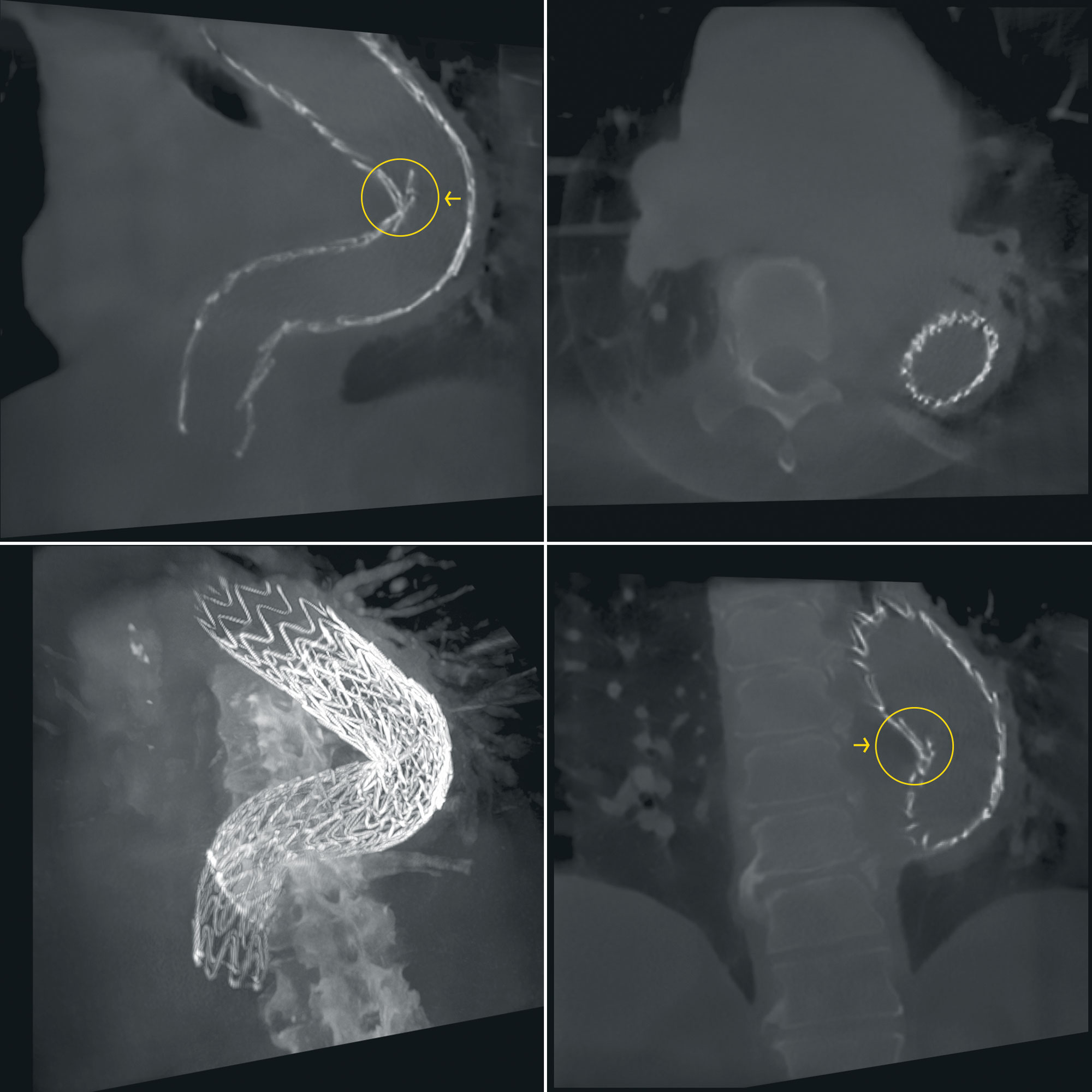
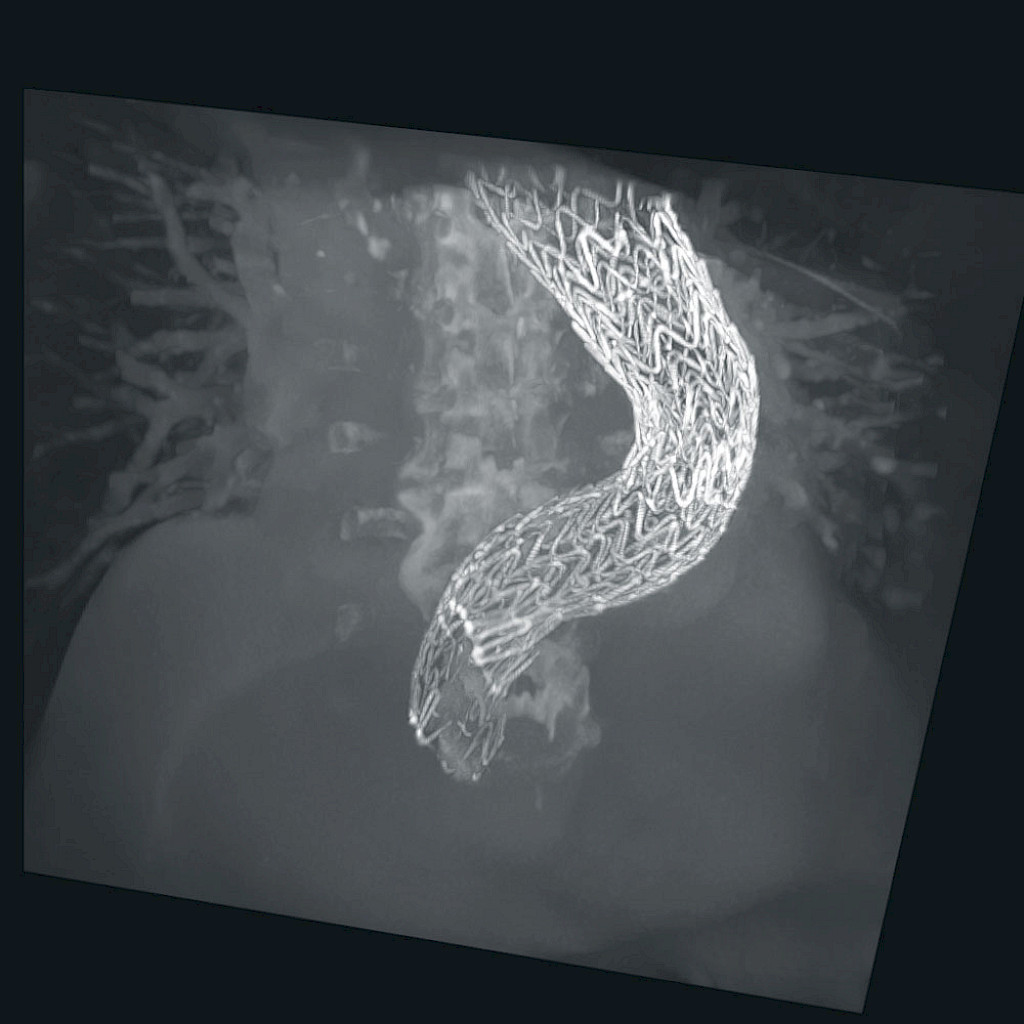
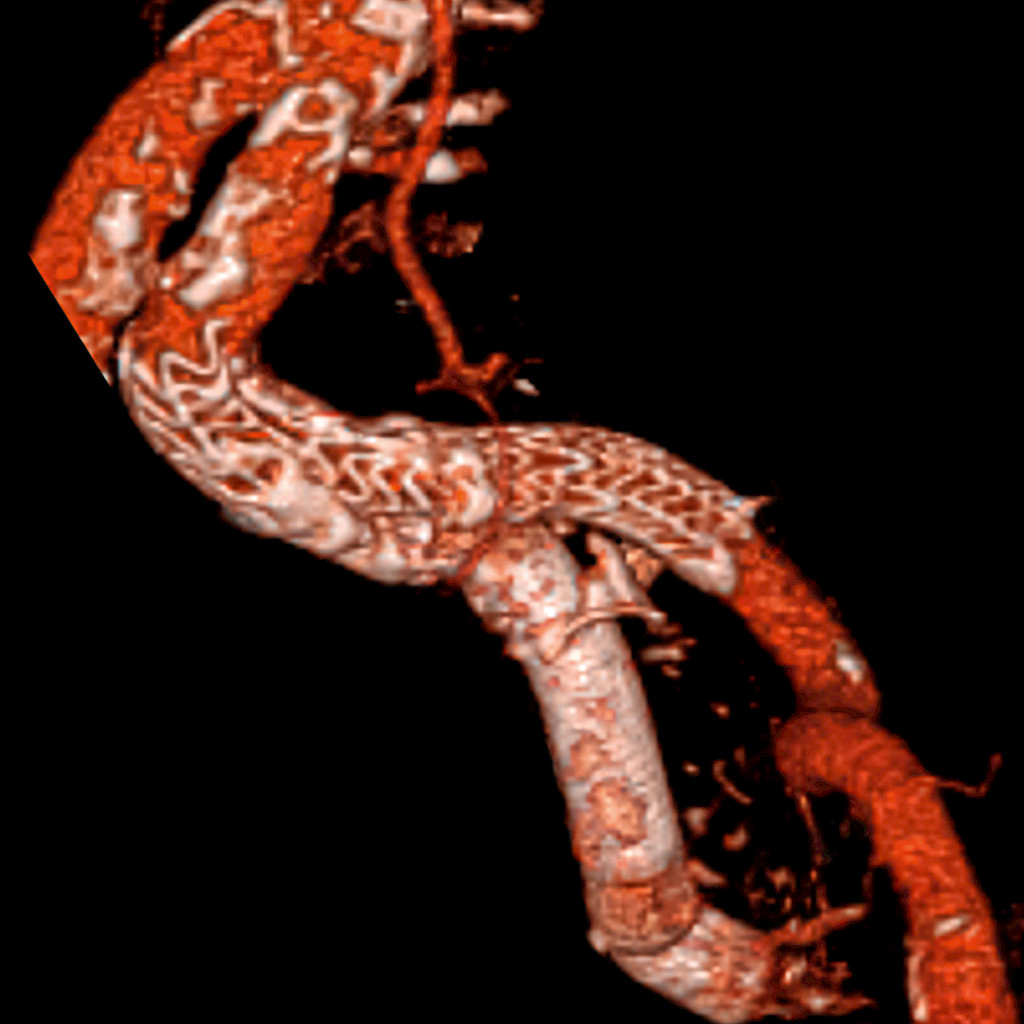
With the mobile 3D C‑arm, Prof. Dr. Veraldi now has a new opportunity: “3D imaging allows us to conduct an intraoperative check on the stent placement. This enables us to confirm whether the stent has unfolded optimally after the vascular procedure has been completed – even while the patient is still under anesthesia. There is no need to wait for the postoperative CT. And we can immediately be sure that we have worked precisely,” says Prof. Dr. Veraldi. This innovative additional step in the EVAR procedure not only enables better surgical results, but is also safer. “If the 3D scan shows that we have to inflate the balloon a little more to achieve perfect results, for example, we can decide this immediately and adapt our surgical procedure accordingly.” A final 3D scan then shows whether the stent is perfectly placed, and the operation can be successfully completed. Thanks to this new treatment method, patients can be discharged from the hospital after just a few days.
“Currently, the postoperative CT scan is regarded as the gold standard for verifying surgical results after an EVAR procedure. The comparison of the intraoperative 3D scan and the postoperative control image from the CT shows us, however, that we now have the same options intraoperatively as postoperatively. This not only makes us more efficient, but also saves lives in extreme cases.”
For Prof. Dr. Veraldi, the 3D scan has become the standard procedure for the treatment of complicated aneurysms. The head of vascular surgery is convinced by the possibility of immediately recognizing whether all measures have been successful, even during challenging operations. “We now have the same options intraoperatively as we otherwise only had in a postoperative CT.”
“Now we can finally see in real time what we used to have to wait several days for.” For Prof. Dr. Veraldi, this is not only an important additional benefit. He thinks that the 3D control scan will help spread and more widely establish the EVAR procedure. The number of open operations, but above all the number of revisions, would decrease significantly as a result. “We can hardly expect more from today’s technology. It offers us an excellent advance in minimally invasive AAA treatment and helps us not only increase our efficiency, but also improve the lives of our patients.”
Disclaimer
1
This product/feature might not be commercially available in all countries. Due to regulatory reasons their future availability cannot be guaranteed. Please contact Ziehm Imaging for detailed information.
More information on Ziehm Vision RFD 3D
—
This clinical story was published in issue 4 (2020).
Download issue 4 as PDF