Learning
from India
Photos
Sameer Raichur

Once considered a Western phenomenon, cardiovascular diseases have become a challenge for the Indian healthcare system. There is an increasing need for cardiological procedures, and most of these are performed in catheter laboratories. Dr. Rajaram Prasad relies on a new concept with a mobile C‑arm for the diagnosis and treatment of coronary heart disease.

Between the Himalayas and the Indian Ocean lies India, the second most populous country in the world. More than 1.37 billion people live here, and population growth continues thanks to progressive modernization and improved healthcare. Western standards are the benchmark for hospitals and practices, and expensive high-end medical technology is finding an increasing number of customers here. But it is not only in this respect that India corresponds with the West. The country is struggling with a growing number of cardiovascular diseases, well-known in the United States and Europe for many years. India plans to master this challenge with so-called ‘cath labs.’ Here, cath labs are more common than in almost any other country. In the big cities, they are multiplying as fast as mushrooms. The term ‘cath lab’ refers to an operating room that requires little equipment and in which only minimally invasive procedures are performed. Open surgery does not take place in cath labs; instead, the small surgical units are used, for example, to insert pacemakers or conduct angioplasties, and minimally-invasive tests.
Wanted: affordable cardiovascular care
Today, many hospitals in India are installing catheterization laboratories. In Salem, a large city 200 kilometers south of Bangalore in the Indian province of of Tamil Nadu, there are more than ten catheterization laboratories alone. One of them belongs to cardiologist Dr. Rajaram Prasad, whose operating room is located in the SIMS Chellum Hospital. Dr. Prasad founded his cath lab in 2018 to ensure better care for his patients. In a public hospital, people are referred from one department to the other and little or no relationship is established with them, says Dr. Prasad. His own catheterization lab, on the other hand, gives him profound patient contact, from diagnosis to treatment. The decision to go into business for himself was not easy for Dr. Prasad. In addition to finding the suitable premises, financing the project was a major challenge. Purchasing high-end medical technology is expensive, and the purchase of a high-quality fixed system, like an X‑ray unit permanently installed in the operating room, which is considered standard imaging in the cath lab, did not seem affordable to Dr. Prasad.


“There are only a few local medical technology manufacturers in India that meet the requirements for cardiovascular interentions. Most systems are imported and are very expensive by our standards,” says Dr. Prasad. He therefore began to think about a ‘mobile cath lab’ in which a mobile high-end C‑arm would replace the fixed system. Initially, he was skeptical as to whether the performance of the mobile system would be sufficient for his needs. Although Dr. Prasad had previously worked with mobile C‑arms from various manufacturers, the results were not always convincing: “Sometimes the image quality was so poor that I could hardly see the arteries. I was able to achieve good results there as well, but at a certain degree of difficulty in the procedure, it became problematic because the images were too noisy.” Dr. Prasad was concerned that a new C‑arm could result in similar image quality issues.
The Ziehm mobile C-arm is known
for its impressive image quality
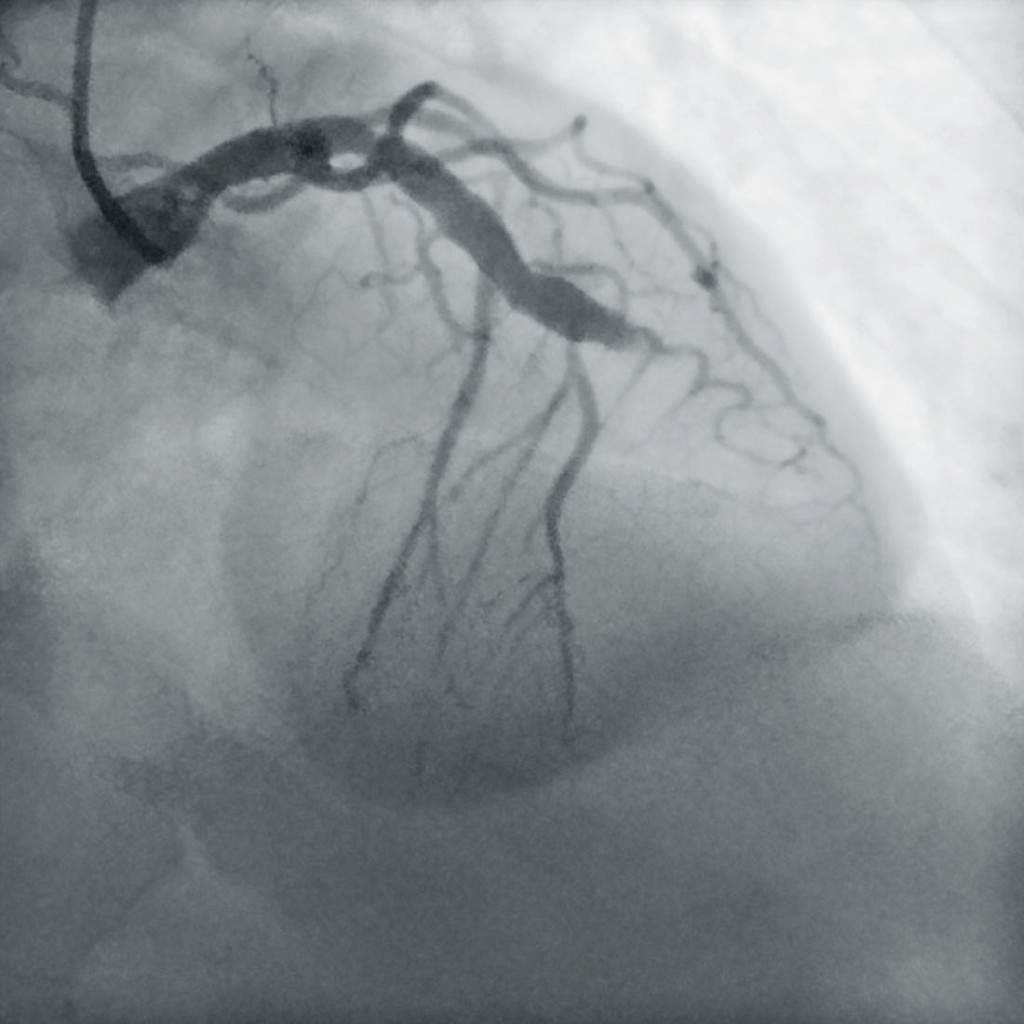
He found the Ziehm Imaging brand during a search for suppliers on the Internet. “My brother is a cardiologist in the USA and warmly recommended the Ziehm system, which is used there in vascular surgery and interventions. He said it was ideal for my procedures,” says Dr. Prasad. He was more than surprised when he visited the Ziehm Vision RFD Hybrid Edition CMOSline1 live in Chennai: “The X‑ray images had a sharpness and accuracy I did not expect from a mobile C‑arm.” Dr. Prasad does not need much space for his mobile cath lab. The C‑arm, an operating table, and a ceiling-mounted monitor, which displays the live and reference X‑ray images as well as the vital functions of the patient, are easily housed in his operating room. There are three people in the operating room for each procedure: Dr. Prasad is supported by a nurse and a cardiovascular technician. He selects his cases carefully, mainly performing primary angioplasty and stenting, which is the treatment of choice for acute myocardial infarction (heart attack). “Since I operate without a surgical backup, I am more careful about selecting my patients for the procedure. I generally refer patients who have triple vessel disease, left main bifurcation, or a complex coronary anatomy to an institution that is better equipped for cardiovascular surgical procedures, as these patients do better with surgical management,” he says.
Mobile versus fixed
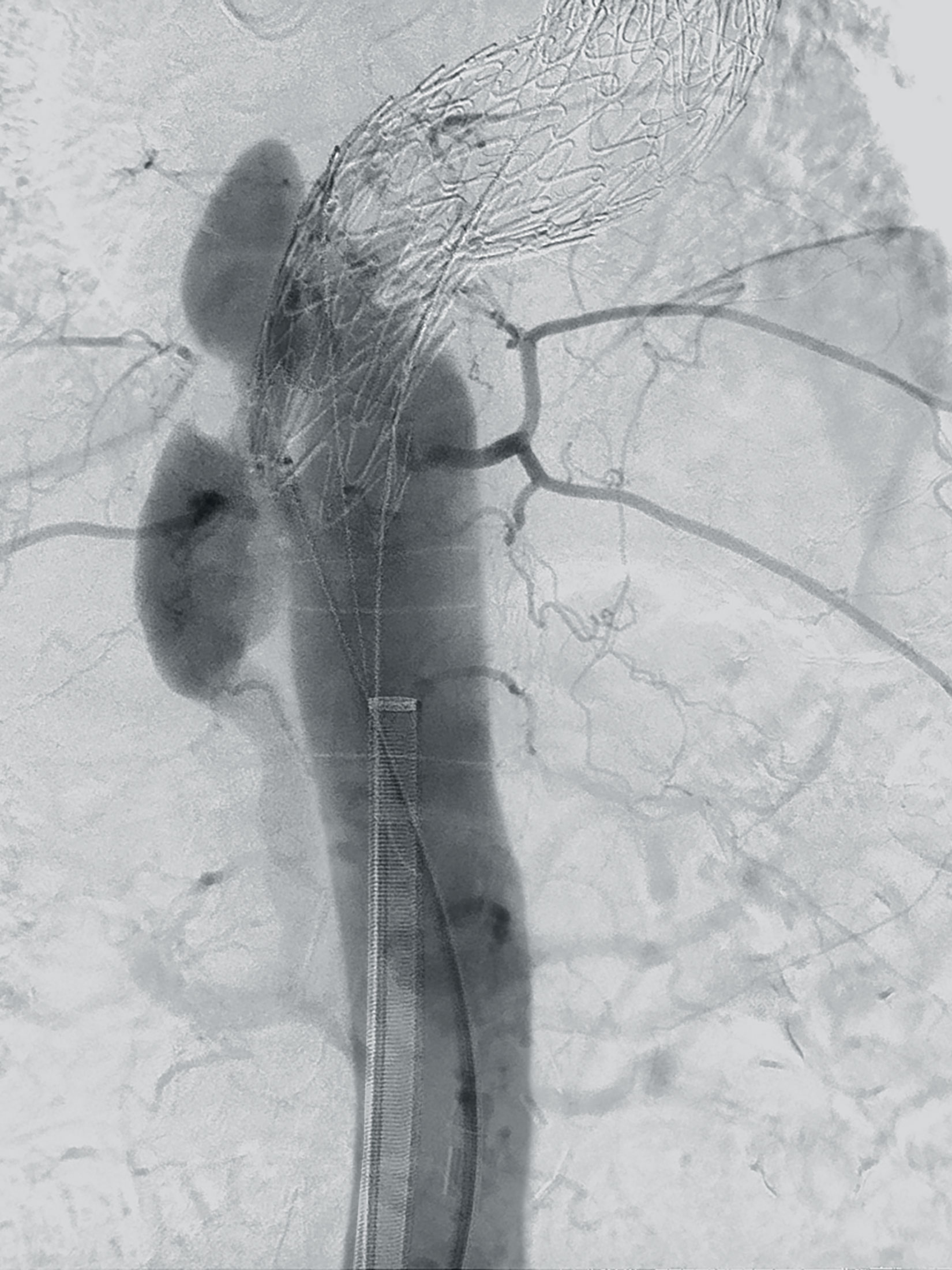
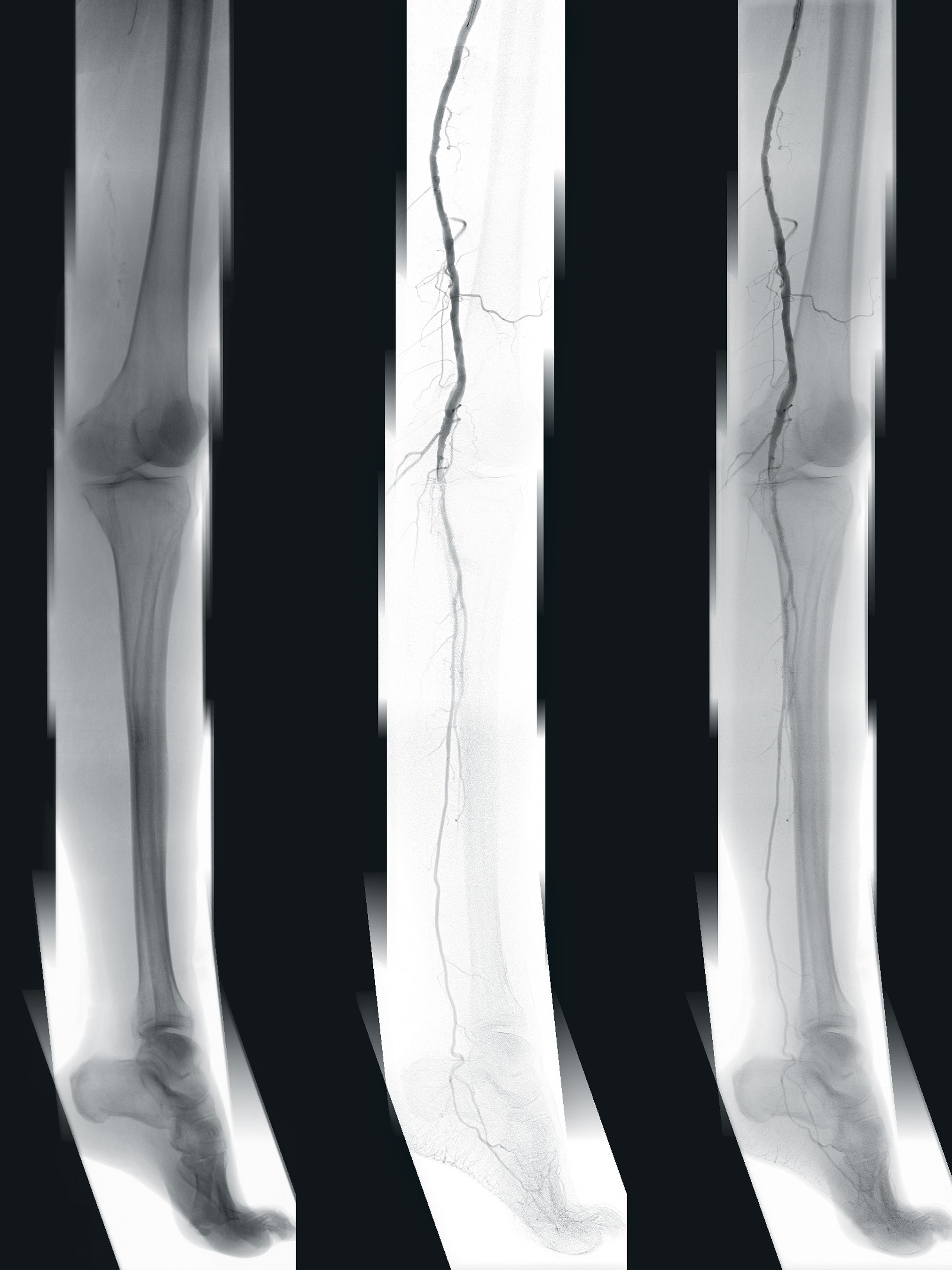
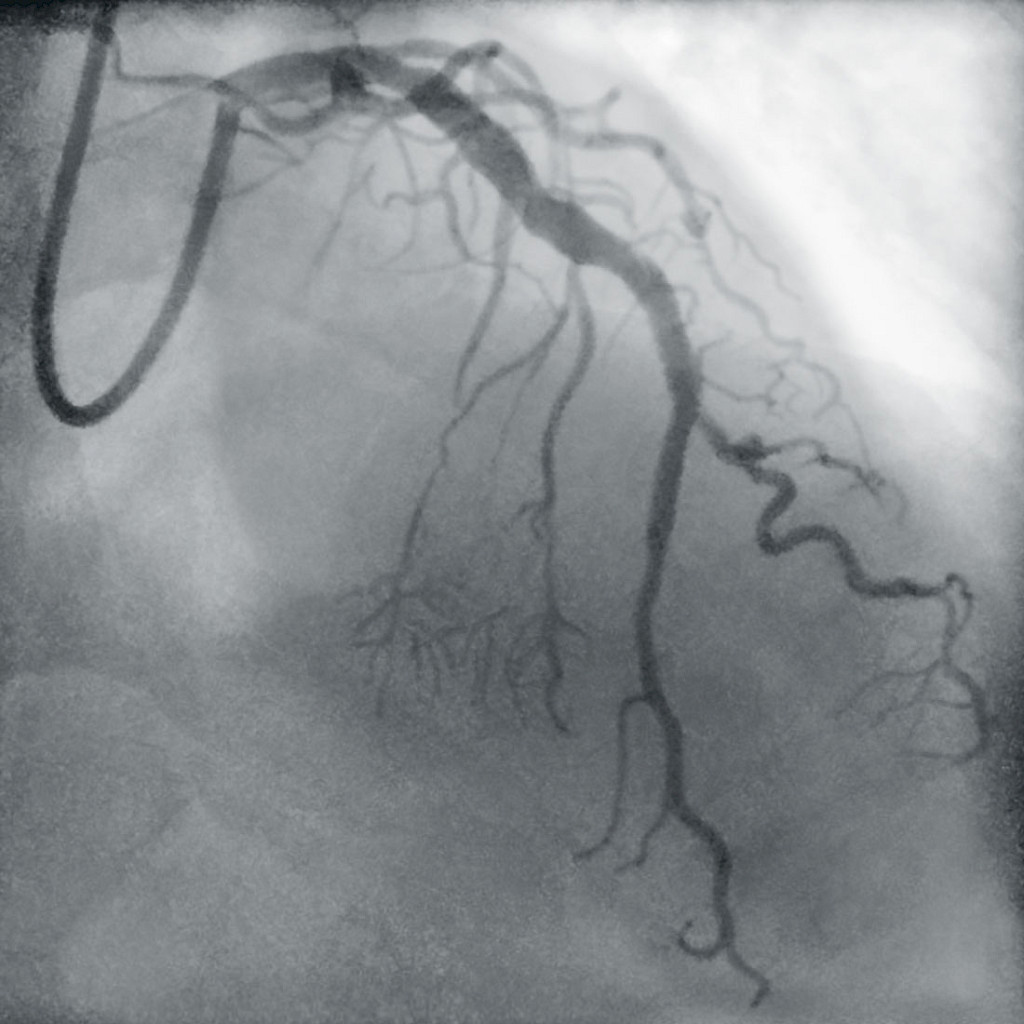
In most cases Dr. Prasad performs an angiogram in the catheter laboratory, i.e., an X‑ray of the vessels with a contrast medium, to examine the condition of the vessels. The most common procedure is angioplasty, in which narrowed or closed vessels are widened or opened again with balloon dilation, followed by stenting. It is precisely these procedures that aroused Dr. Prasad’s interest in cardiology. “Angiograms fascinated me from the beginning of my training. You can see exactly what you did and if you were successful. Good imaging is very important to me because it allows me to measure my results exactly,” says Dr. Prasad. For him, it makes no difference whether the images are taken by a fixed system or by his mobile C‑arm: “People should not judge the image quality just because it is a mobile C‑arm. Initially, I was also skeptical as to whether the image quality could compete with that of a fixed installation. If my colleagues saw the X‑rays I acquire in my mobile cath lab, they would think differently. The image quality I get with my C‑arm is as good as that of a fixed system and definitely better than any image taken with a low-cost fixed system.”

The mobile cath lab has proven to be the right choice for Dr. Prasad. Not only are the acquisition costs of a mobile system lower than those of a fixed installation, but also the maintenance costs, he says: “For fixed installations you need a high-capacity power supply, which of course costs money. My electricity costs for the mobile cath lab are significantly lower than what I would have with a standard cath lab.” In addition, installing a fixed system would require structural changes that are not necessary with his mobile concept. The personnel costs are also manageable, as he only needs an assistant and a cardiovascular technician. Another positive side-effect for Dr. Prasad is the dose-saving work in the operating room, which is very important to him: “It is not possible to estimate the amount of radiation my team is exposed to. That’s why it is crucial to have medical technology that is as dose-saving as possible. Ziehm Imaging’s C‑arm with a CMOS detector is the answer for me.”

When asked whether the mobile cath lab has limitations, Dr. Prasad shakes his head: “Our mobile concept has only advantages for me, my employees, and my patients. I haven’t had a case that I could have solved better with a fixed system.” For him, the mobile cath lab is a model for the future. “Medical imaging is becoming more and more important for us, and it is getting better every day. If we can afford the latest technology, everyone wins.”
Disclaimer
1
The CMOSline is a system configuration based on the Ziehm Imaging CMOS flat-panel detector.
More information on SIMS Chellum Hospital
More information on Ziehm Vision RFD Hybrid Edition
—
This clinical story was published in issue 4 (2020).
Download issue 4 as PDF